

Introduction
The prostate gland is situated beneath the urinary bladder and it encircles the urethra, the tube along the penis through which urine flows from the bladder. It contains glands, muscles and fibrous tissue. As part of the male reproductive system it produces part of the semen which nourishes, lubricates and transports sperm during ejaculation.
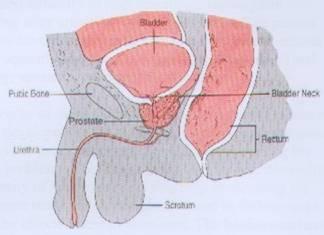
Cross section of the prostate gland
Benign prostatic hyperplasia (BPH)is a non-cancerous enlargement of the gland occurring most commonly in men over 50 years old. The prevalence of BPH is greater than 50% at age 60 years old and in men over 85 years old it is more than 90%. It is an important disease because it produces urinary symptoms which are bothersome and affects the patient’s lifestyle and sleep.
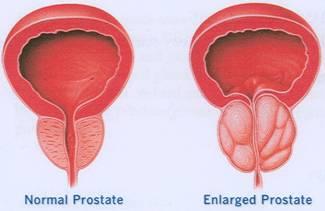
Benign prostatic hyperplasia
Signs & symptoms
The symptoms occurring in BPH are not exclusive or specific to this condition and may be found in other diseases of the lower urinary tract eg bladder cancer, bladder stones, urinary tract infection, prostate cancer, infection of prostate, urethral obstruction. Obstructive symptoms include poor stream of urine, straining to urinate, hesitancy (difficulty to start urinating), incomplete emptying after urinating, interrupted stream. The patient may also have irritative symptoms causing him to urinate more frequently (daytime and night time frequency) and urgency (sensation of urgent need to urinate).
The severity of these symptoms is assessed using a scoring system developed by the American Urological Association whereby the patient answers 7 questions concerning his urinary problems. The final score added up will determine the severity of his disease and also help in choosing the appropriate treatment. It can also be used in follow-up to assess the effectiveness of treatment. The bothersomeness of his symptoms affecting his life is scored using the Quality of Life (QOL) score.
Some patients with large prostate glands may have few or no symptoms while others with smaller glands may have severe symptoms. Patients may suddenly present with inability to urinate and develop acute urinary retention. This can be precipitated by taking medications for the common cold e.g. decongestant.
Digital rectal examination (DRE)
The doctor performs a DRE to diagnose BPH whereby he inserts a lubricated and gloved finger into the patient’s rectum. An enlarged gland that is smooth and soft is most likely due to BPH. A hard and nodular gland may signify infection of the prostate (prostatitis) or even cancer of the prostate.

Digital rectal examination
Other tests
Your doctor may perform a blood test to check PSA (prostate specific antigen) levels. This protein is secreted by the prostate gland and is found in the blood. When levels are elevated beyond normal, a TRUS (transrectal ultrasound) biopsy of the prostate is performed to exclude prostate cancer (see section in Prostate Cancer). A large gland with BPH and infection of the prostate (prostatitis) can also cause elevation of PSA.
A sample of urine is examined microscopically to look for evidence of bleeding and infection. A patient also undergoes a urine flow (UROFLOW) study where he passes urine into an apparatus which measures the speed of urine flow which may be prolonged in BPH.
An x-ray of the abdomen is also taken to look at the bladder as it is known that there is a higher occurrence of bladder stones with BPH among Malaysian men.
Complications
Infection of the bladder may occur because of obstruction and repeated infections encourage the formation of bladder stones. This infection may spread to the testicles. A very large gland which is vascular can cause bleeding and sometimes clots completely block the urinary passage.
Long standing obstruction may affect both kidneys causing them to swell. In this situation the patient has urinary retention but does not suffer any pain unlike the situation where he has acute urinary retention. Kidney function is affected and the patient eventually develops kidney failure unless the obstruction is relieved.
The bladder wall muscle has to contract harder to overcome the prostatic obstruction and over time it will thin out and the patient develops failure of his bladder muscle to contract.
Treatment
BPH can be treated medically or surgically. The doctor takes into consideration the severity and bothersomeness of symptoms, presence of complications, patient’s age and lifestyle before deciding on the appropriate treatment. However in patients with very few symptoms which do not bother them, “watchful waiting” is offered. They are not given any form of treatment but rather followed up regularly to monitor their symptoms.
Medical Treatment
This form of treatment is increasingly used as many patients prefer to avoid surgery. However medication need to be taken lifelong and significant side-effects may occur. Basically there are 2 major groups, alpha-l- blockers and 5-alpha reductase inhibitors.
Alph-1-blockers
These drugs relax smooth muscle in the prostate and bladder neck, thereby improving urine flow. Examples include Terazosin (Hytrin), Doxazosin(Cardura) and Alfuzosin (Xatral). The benefits of alpha-I-blockers may be seen within a few days to 2 weeks. However a significant side-effect is a sudden drop in blood pressure initially. Patients may complain of feeling giddy or light headed especially on getting up from bed or from a chair. Therefore patients are advised to take these medications at bedtime. However certain drugs have special formulations to reduce this side-effect.
5-alpha Reductase Inhibitors
These drugs partially shrink the prostate gland by inhibiting the enzyme 5-alpha reductase that is needed to convert testosterone to dihydrotestosterone which is necessary for prostate growth. It takes almost 6 months before any effect is noticed. Examples of drugs in this group include Finasteride(Proscar) and Dutasteride (Avodart). Side effects include impotence, loss of libido and reduced volume of ejaculate.
Surgical Treatment
The most common surgical procedure for the treatment of BPH is transurethral resection of the prostate (TURP). This procedure performed under spinal anaesthesia by an urologist, involves insertion of an instrument called a resectoscope. The urologist then proceeds to remove the prostatic tissue to create a larger channel for the patient to urinate. It takes about I hour to perform this surgery and the patient usually needs to stay 3 days. A very large gland may need to be removed by an open operation under anaethesia called prostatectomy, through an incision in the lower abdomen.
Common complications of surgery include bleeding and infection. In TURP many men may experience retrograde ejaculation whereby instead of semen flowing out during ejaculation, it flows back into the bladder. Rarely a patient may lose bladder control either temporarily or permanently. Difficulty in achieving erection is rare after surgery.
While surgery results in an immediate reduction in symptoms, there is a possibility of regrowth of the prostate causing obstruction in about 5% of patients.
Other alternatives to TURP include using laser, microwave and heat therapy. Some patients who have failed medical therapy but are not fit for surgery may undergo insertion of a prostatic stent, a device like a spring which opens up the narrowed utrehra.
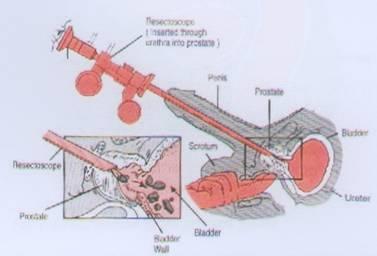
Transurethral Resection of Prostate (TURP)
Support
Malaysian Urological Association (MUA) – www.urology-malaysia.org
National Institute of Diabetes and Digestive and Kidney Disease – www.kidney.niddk.nih.gov
| Last Reviewed | : | 26 April 2012 |
| Writer | : | Dr. Susan Woo |
| Reviewer | : | Dr. Sunita a/p Bavanandan |





